GERD (Gastroesophageal reflux disease) is a chronic digestive disorder characterized by the backward flow of stomach contents into the esophagus, leading to troublesome symptoms and potential complications. While occasional acid reflux is common and usually harmless, GERD represents a persistent condition that can significantly impair quality of life and increase the risk of esophageal injury if left untreated. With changing dietary habits, sedentary lifestyles, rising obesity rates, and increased stress, the prevalence of GERD has grown globally, making it one of the most common gastrointestinal disorders encountered in clinical practice today.
Understanding GERD
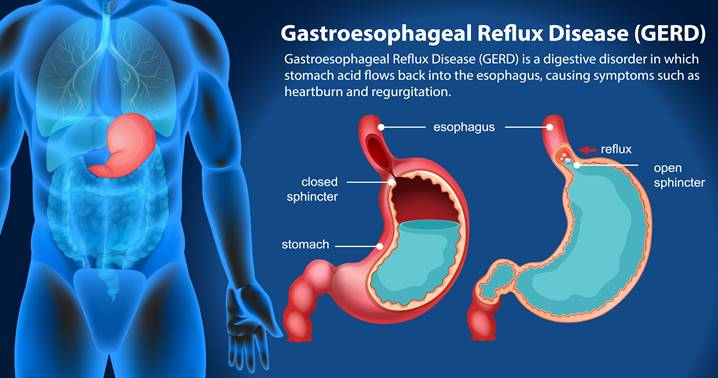
GERD develops when the lower esophageal sphincter (LES), a ring of muscle located between the esophagus and stomach, fails to function properly. Under normal circumstances, the LES relaxes to allow food into the stomach and then tightens to prevent gastric contents from flowing backward. In GERD, this barrier becomes weak or relaxes inappropriately, allowing acid, digestive enzymes, and bile to reflux into the esophagus.
The esophageal lining is not designed to withstand repeated acid exposure. Over time, this can lead to inflammation, mucosal damage, and structural changes. Unlike occasional acid reflux, which may occur after heavy meals or alcohol intake, GERD is defined by frequent symptoms or objective evidence of esophageal injury, making it a chronic and clinically significant condition.
Causes of GERD
GERD is a multifactorial disease influenced by lifestyle habits, dietary choices, anatomical abnormalities, and underlying medical conditions.
Lifestyle-Related Causes
Lifestyle factors play a central role in the development and progression of GERD. Overeating increases gastric pressure, making reflux more likely, especially when meals are consumed late at night. Lying down soon after eating reduces the effect of gravity that normally helps keep stomach contents in place. Obesity is a major risk factor, as excess abdominal fat increases intra-abdominal pressure, promoting reflux and impairing LES function.
Smoking contributes to GERD by reducing LES tone and impairing saliva production, which normally helps neutralize acid. Alcohol consumption further relaxes the LES and increases gastric acid secretion. Physical inactivity and chronic stress also contribute indirectly by affecting digestion, hormone balance, and eating behaviors.
Dietary Triggers
Certain foods are known to exacerbate GERD symptoms by increasing acid production or relaxing the LES. Fatty and fried foods slow gastric emptying, allowing acid to remain in the stomach longer. Spicy foods may irritate the esophageal lining, intensifying discomfort. Caffeine, chocolate, peppermint, and carbonated beverages reduce LES pressure, increasing the likelihood of reflux.
Acidic foods such as citrus fruits and tomato-based products can worsen symptoms by directly irritating inflamed esophageal tissue. Large portion sizes and highly processed foods further compound these effects, especially when combined with poor meal timing.
Medical and Physiological Factors
Several medical conditions contribute to GERD pathophysiology. Hiatal hernia, a condition in which part of the stomach protrudes through the diaphragm into the chest cavity, disrupts the normal anatomy of the LES and promotes reflux. Pregnancy increases GERD risk due to hormonal changes that relax smooth muscles and mechanical pressure from the growing uterus.
Certain medications, including nonsteroidal anti-inflammatory drugs (NSAIDs), calcium channel blockers, anticholinergics, and some antidepressants, can worsen reflux by reducing LES tone or irritating the esophagus. Delayed gastric emptying, connective tissue disorders, and neurological conditions affecting swallowing also increase susceptibility.
Common Symptoms of GERD
GERD presents with a wide range of symptoms, which can be digestive or extra-esophageal in nature.
Digestive Symptoms
Heartburn is the most common symptom of GERD and is described as a burning sensation behind the breastbone that often worsens after meals or when lying down. Acid regurgitation, characterized by a sour or bitter taste in the mouth, occurs when stomach contents reach the throat or oral cavity. Chest discomfort related to GERD can mimic cardiac pain, making an accurate diagnosis essential.
Other digestive symptoms include bloating, nausea, excessive belching, and a feeling of fullness after small meals. Difficulty swallowing may occur as inflammation progresses.
Non-Digestive (Atypical) Symptoms
GERD frequently causes extra-esophageal symptoms that are often overlooked. Chronic cough, throat clearing, hoarseness, and sore throat result from repeated acid exposure to the larynx and pharynx. Some individuals experience asthma-like symptoms or worsening respiratory conditions due to microaspiration of gastric contents.
A sensation of a lump in the throat, known as globus sensation, and dental enamel erosion are also recognized manifestations. These atypical symptoms can occur even in the absence of classic heartburn, complicating diagnosis.
Potential Complications of Untreated GERD
When GERD is left untreated or poorly managed, chronic acid exposure can lead to serious complications. Esophagitis, or inflammation of the esophageal lining, is a common early consequence and may progress to erosions or ulcers that cause pain and bleeding. Repeated injury can result in scar formation and strictures, leading to persistent swallowing difficulties.
One of the most concerning complications is Barrett’s esophagus, a condition in which normal esophageal cells are replaced with abnormal, intestinal-type cells as an adaptive response to acid exposure. Barrett’s esophagus significantly increases the risk of esophageal adenocarcinoma, highlighting the importance of early detection and long-term management.
Diagnosis of GERD
GERD diagnosis is often based on clinical symptoms and response to acid-suppressive therapy. In patients with alarm symptoms such as difficulty swallowing, unintentional weight loss, gastrointestinal bleeding, or persistent symptoms despite treatment, further evaluation is required.
Upper gastrointestinal endoscopy allows direct visualization of the esophageal lining and detection of inflammation, ulcers, strictures, or Barrett’s changes. Ambulatory pH monitoring measures acid exposure in the esophagus and is considered the gold standard for confirming GERD in uncertain cases. Esophageal manometry may be used to assess motility disorders when surgical intervention is considered.
Management and Treatment of GERD
Effective GERD management involves a combination of lifestyle changes, dietary modification, pharmacological therapy, and, in select cases, surgical intervention.
Lifestyle Modifications
Lifestyle changes form the cornerstone of GERD management and are recommended for all patients. Eating smaller, more frequent meals reduces gastric pressure. Avoiding lying down for at least two to three hours after eating helps prevent reflux. Elevating the head of the bed during sleep reduces nocturnal symptoms by using gravity to limit acid exposure.
Weight loss is strongly associated with symptom improvement in overweight individuals. Smoking cessation and limiting alcohol intake further enhance LES function and reduce mucosal irritation.
Dietary Management
Dietary strategies focus on minimizing trigger foods while maintaining balanced nutrition. A GERD-friendly diet emphasizes whole grains, lean proteins, vegetables, non-citrus fruits, and healthy fats in moderate amounts. Meal timing is critical, as late-night eating significantly worsens reflux.
Adequate hydration supports digestion, but excessive fluid intake during meals may increase gastric distension. Personalized dietary adjustments based on symptom response are often more effective than rigid elimination diets.
Medications
Pharmacological therapy is widely used to control GERD symptoms and heal esophageal damage. Antacids provide rapid, short-term relief by neutralizing stomach acid. H2 receptor blockers reduce acid production and are effective for mild to moderate symptoms.
Proton pump inhibitors (PPIs) are the most potent acid-suppressive medications and are considered first-line therapy for moderate to severe GERD. When used appropriately under medical supervision, PPIs promote mucosal healing and reduce complication risk. Long-term use requires periodic reassessment to balance benefits and potential risks.
Medical and Surgical Options
For patients with severe, refractory GERD or complications despite optimal medical therapy, surgical options may be considered. Fundoplication, which reinforces the LES by wrapping the upper stomach around the esophagus, has demonstrated long-term efficacy in selected patients. Emerging endoscopic therapies offer minimally invasive alternatives in specific cases.
Bottom Line
GERD is a chronic but manageable digestive disorder influenced by lifestyle, diet, and physiological factors. Early recognition and evidence-based management are essential to prevent complications and improve quality of life. Through a combination of healthy habits, appropriate medical therapy, and regular monitoring, most individuals with GERD can achieve effective symptom control and long-term digestive health.
- Written By: Shabina Khan (Clinical Pharmacist)
- Medically Reviewed By: Dr Avinash Singh (PhD, Pharm. Medicine)